Castellano | Euskara | Français | English

DAR No 3: Agomelatine (Valdoxan ®)
Share it





Worse than first-line antidepressants, up to 15-fold more expensive, and a worrying hepatic safety profile
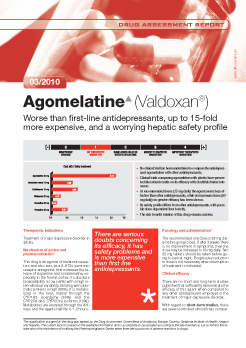
- No clinical trial has been undertaken to compare the antidepressant agomelatine with other antidepressants.
- Clinical trials comparing agomelatine with placebo have presented discordant results on its efficacy with doubtful clinical relevance.
- At recommended doses (25 mg daily) the agent seems less effective than other antidepressants, while at maximum doses (50 mg daily) no greater efficacy has been shown.
- Its safety profile differs from other antidepressants, with possible dose-dependent liver toxicity.
- The risk-benefit relation of this drug remains unclear.
- See readers’ comments at the bottom of this page (2 COMMENTS!!)
- COMMENT 1
- Regarding to the agomelatin assessment report we disagree in two aspects and thereby kindly ask you for correction:
- 1- It is stated that "agomelatin is no better than placebo". Valdoxan has proved to be more effective than placebo, which is a necessary condition for approval to be granted by the EMA and the Spanish Ministry of Health.
- 2- The expression “at the price of gold” is a figure of speech used in colloquial language, is not technical and is subjective as well. It is not adequate in the context of a technical assessment report published in the website of an official institution
- We kindly request you to consider both aspects and make the timely corrections in your website as soon as possible.
- Sincerely, J L Zaldívar
- Competing interests: Servier Laboratories employee
- Full name: Juan Luis Zaldívar Hernández
- Occupation: Assistant Director of Institutional Policies.
- Place of work: MADRID
- Date: June 1st, 2010.
- AUTHORS´ REPLY
- 1- After assessing the current evidence on agomelatine, including both published and unpublished clinical trials, the Navarre Committee on New Drugs Assessment (NCNDA) agrees with the view of two members of the EMA(1) in terms of considering the efficacy of the drug versus placebo as unclear or inconsistent. In more than 50% of the trials the efficacy of agomelatine was not superior to placebo. In line with these two EMA experts’ opinion, we also think that agomelatine should have not been granted approval until its efficacy had been more consistently proved.
- Moreover, other independent assessments draw a similar picture to that in our report. For example, the French Journal La Revue Prescrire(2) states that “agomelatine has not proven efficacy yet”. The British MTRAC (Midlands Therapeutic Review and Advisory Committee)(3) states that “agomelatine cannot be recommended for prescribing because the current evidence for its efficacy and safety is inadequate to support its use. Agomelatine has not consistently been found to be more effective than placebo in the treatment of depression”. The NHS Scottish Medicines Consortium(4) states that “there are still a number of uncertainties around the use of agomelatine including the lack of consistently demonstrated clinical benefit, the magnitude of that benefit, and whether increasing the dose to 50 mg offers additional benefit”. The Scottish NHS advises against prescribing agomelatine.
- Though we do not find any sound argument to take it for granted that agomelatine has proven to be more effective than placebo the drug was granted EMA approval. Challenging the efficacy of agomelatine versus placebo might contradict the fact of it having been launched into the market. However this is consistent with a rigorous scientific approach.
- Now it may be more important to stress the point that agomelatine seems to be less effective than the first-line antidepressants. According to the available evidence, when used at habitual doses, agomelatine seems to be less effective than first-line antidepressants, and it has not proved to be more effective at the maximum doses when compared to habitual doses.
- 2- With regard to the expression “at the price of gold” we assume that it is a figure of speech to let the reader know that the cost of the treatment is excessively high. However, apart from catching the reader’s eye on a very important point which is the economic impact, detailed information about comparative prices with other antidepressants is given.
- Moreover, had we been quite strict on this point we should have stated that “agomelatine is more expensive than gold”. According to the London Gold Fixing (www.goldfixing.com), the price of pure gold on June 1st 2010 was 32.26 euros per gram while that of agomelatine is 85.86 euros per gram.
- However we decided to have the expression “up to 15-fold more expensive” written in the subtitle in order to show a more precise information on the disproportionate price of the drug, given that agomelatine seems to be less effective than first-line antidepressants and its efficacy versus placebo has not been consistently proved.
- Thereby the NCNDA agrees to replace the subtitle “No better than placebo with a worrying hepatic safety profile, and at the price of gold” for “Worse than first-line antidepressants, up to 15-times more expensive, and a worrying hepatic safety profile”.
- (1) Informe EMEA. EPAR: http://www.emea.europa.eu/humandocs/PDFs/EPAR/valdoxan/H-915-en6.pdf
- (2) Agomelatina. Efectos adversos y eficacia no probada. Rev Prescrire September 2009;29(311):646-650
- (3) Agomelatine for the treatment of major depressive episodes. MTRAC http://195.62.199.219/pctsla/mtrac/productinfo/verdicts/A/Agomelatine.pdf (accedido el 02/06/2010)
- (4) National Health Service. Scottish Medicines Consortium. Agomelatine, 25 mg film-coated tablets (Valdoxan) (No.564/09)http://www.scottishmedicines.org.uk/files/agomelatine%20(Valdoxan)%20FINAL%20Oct%202009%20Revised%20041109.doc%20for%20website.pdf (accedido el 02/06/2010).
- COMMENT 2
- Let me first express my gratitude for the opportunity to comment on your article. I worked for Servier Laboratories on the promotion of agomelatine and would like to ask you some questions. I used to give doctors offprints of clinical studies that proved agomelatine effective when compared with venlafaxine, sertraline and fluoxetine as well. Maybe I was not giving the right information to doctors or you are not very well informed instead.
- Secondly, I think that the EMA recommends that all new antidepressants carry a warning on their possible hepatic side effects, is that correct? Lastly, I want to state that I do not like speaking badly of any drug unless there is compelling evidence for that. Nowadays if I had to choose the best antidepressant in my opinion escitalopram is the one according to doctors’ clinical experience.
- In summary, agomelatine should be given an opportunity to really show whether it does the trick, and then we will come to know whether one gram of agomelatine makes patients get their money worth as gold or escitalopram do.Looking forward to hearing from you. Let me congratulate you for your rigorous and good job.
- Sincerely,
- Gonzalo Arévalo.
- Competing interests: Servier Laboratories employee
- Full name: Gonzalo Arévalo.
- Occupation: Servier Laboratories’ sales representative
- Place of work: MEXICO
- Date: July 26th, 2010.
- AUTHORS’ REPLY
- Publication bias is one of the main difficulties concerning agomelatine assessment. As mentioned in our report, trials with positive results have been published in different medical journals while those with negative outcomes remain unpublished. In this case, data can only be consulted at the EMA Public Assessment Report. After a thorough search of agomelatine trials we identified the following:
- a)Two trials comparing agomelatine vs venlafaxine (references 7 and 8 in our report). The primary endpoint in these studies was not the efficacy of the drugs as antidepressants but the outcomes on sleep disorders and sexual activity instead. Both trials were underpowered and no conclusion can be obtained on the comparative efficacy of the drugs as antidepressants. This is also stated in the EMA assessment report (page 45). Therefore, these trials cannot validly answer the clinical question on whether agomelatine is as effective as venlaxafine in the management of depression. They may however be useful to boost the sale of agomelatine.
- b)Another trial compared agomelatine vs sertraline in which the primary endpoint was the outcomes on the rest-activity cycle. Again the efficacy of the drug as an antidepressant is not assessed and no information can be obtained on whether agomelatine is as effective as sertraline in the treatment of depression. To answer this question it would be necessary to carry out a well powered and designed non-inferiority trial. So far this information is still lacking. In the EMA assessment report this trial is mentioned as a small study that should not be included when evaluating agomelatine efficacy as antidepressant.
- c)Three trials comparing agomelatine vs placebo including an arm with an active drug (fluoxetine 20 mg, two trials; and paroxetine 20 mg, one trial). In this case the primary endpoint was the efficacy of the drug as an antidepressant. All these trials remain unpublished. In all three studies agomelatine did not prove better than placebo. In two of them the active compared agents (fluoxetine and paroxetine) did not obtain better results than placebo either, except in one study where fluoxetine did. According to the EMA assessment report (only available source of information), agomelatine´s efficacy seems to be lower than fluoxetine 20 mg which is reflected in our report.
- Let us remind you that in our assessment report we selected the trials that evaluated agomelatine´s efficacy as an antidepressant only. With respect to the comment on the EMA recommending that all new antidepressants carry a warning regarding their possible hepatic side effects, let us clarify that the EMA does not require that on a regular basis. In the case of agomelatine the alert was specifically included along with the requirement of close monitoring of liver function due to the higher incidence of hepatic disorders related to the drugs use, including severe cases of hepatic impairment (see EMA assessment report).
- We think drugs should be given an opportunity to be tested in clinical practice provided they have already proved through well-designed clinical trials to be at least as effective and safe as other marketed drugs. We should also bear in mind that trials’ characteristics may differ from conditions in clinical practice. Therefore a favourable risk/benefit balance should be observed for a drug to be authorized which does not seem to be the case of agomelatine given the available evidence.
- After publishing our report more information on agomelatine has been released from two new clinical trials. The first study (1) assessed the efficacy in depression of agomelatine 25 and 50 mg daily vs placebo during an 8 week period (HDRS-17 score as primary outcome). Agomelatine 25 mg was better than placebo but the 50 mg dose was not. The authors concluded that “agomelatine 25 mg/d was effective in the treatment of patients with moderate-to-severe MDD and was safe and well tolerated. Agomelatine 50 mg/d provided evidence for its antidepressant efficacy until week 6 and was also safe and well tolerated”. Surprisingly, the authors never mentioned that the 50 mg dose was no better than placebo.
- The second trial (2) had a similar design. A total of 511 patients were randomized to receive either agomelatine 25 mg, 50 mg or placebo. No differences were observed between agomelatine 25 mg and placebo although the 50 mg dose was significantly better than placebo. The higher dose was also associated with aminotransferase elevations in 4.5% of the patients. The authors concluded that “the results showed significant antidepressant efficacy of agomelatine 50 mg/d, including a positive effect on sleep compared with placebo in outpatients with moderate to severe major depressive disorder”. Surprisingly, the authors never mentioned about the lack of efficacy of the 25 mg dose.
- What conclusion can we reach about the efficacy of agomelatine vs placebo? Unfortunately, the question still remains unanswered.
- (1) Stalh et al. Agomelatine in the treatment of major depressive disorder: an 8-week, multicenter, randomized, placebo-controlled trial. J Clin Psychiatry 2010;71:919-626.
- (2) Zajecka J et al. Efficacy and safety of agomelatine in the treatment of major depressive disorder: a multicenter, randomized, double-blind, placebo-controlled trial. J Clin Psychophramacol. 2010;30:135-144.